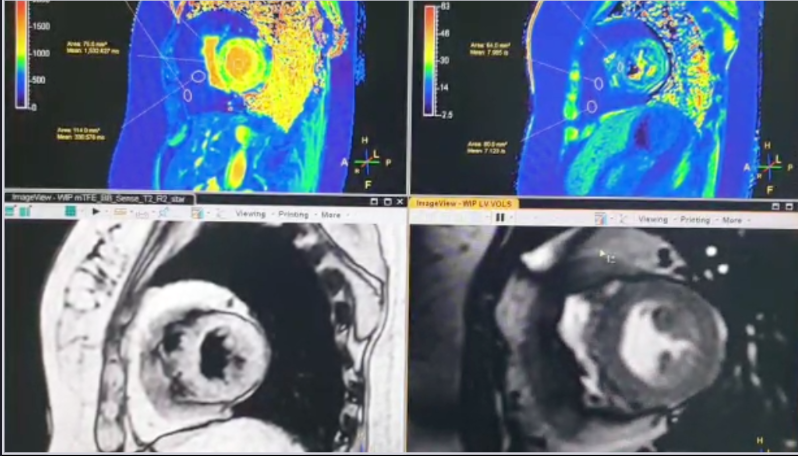
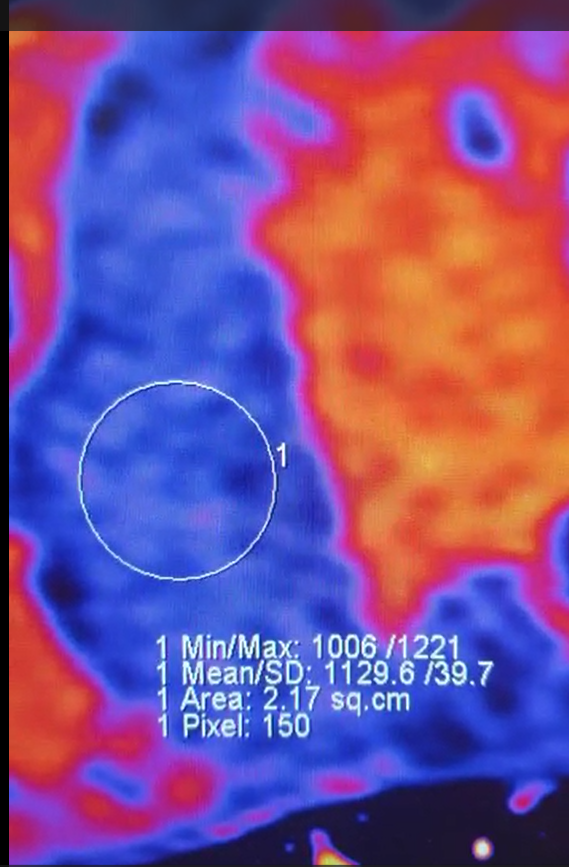
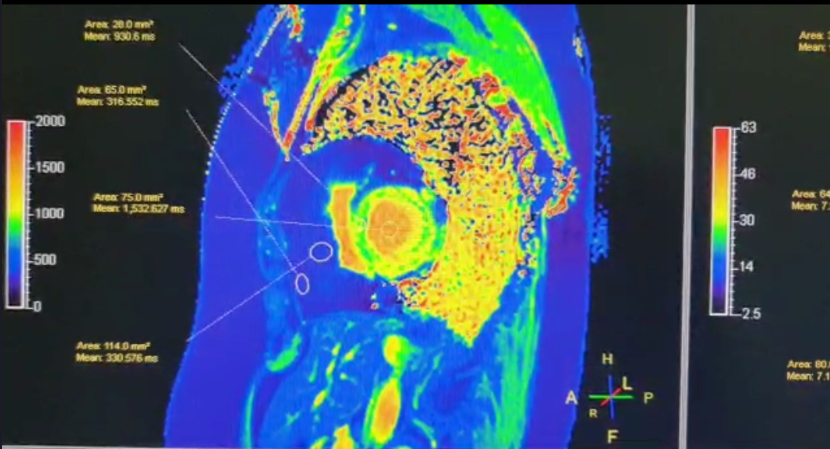
Value of parametric imaging in CMR
Hybrid EPI Sequence for Adenosine Stress Perfusion Cardiac MRI on 1.5T Siemens Aera.
A lot of centres using Siemens scanners have moved to the Hybrid EPI sequence with motion correction (MOCO) because of its perceived low susceptibility to dark rim/Gibbs artefact- this is still present though. CNR tends to be significantly higher than the FLASH sequence whilst SNR is comparable. Ischaemia detection is subjective, but with the majority of our clinicians preferring the EPI to the FLASH Sequence. Best to do with a phase encoding direction of head-foot and free breathing stress becomes easily achievable- the MOCO takes care of the rest. Quite grainy (EPI), but still good at detecting inducible ischemia sites. Spatial and temporal resolution is comparable with the FLASH.
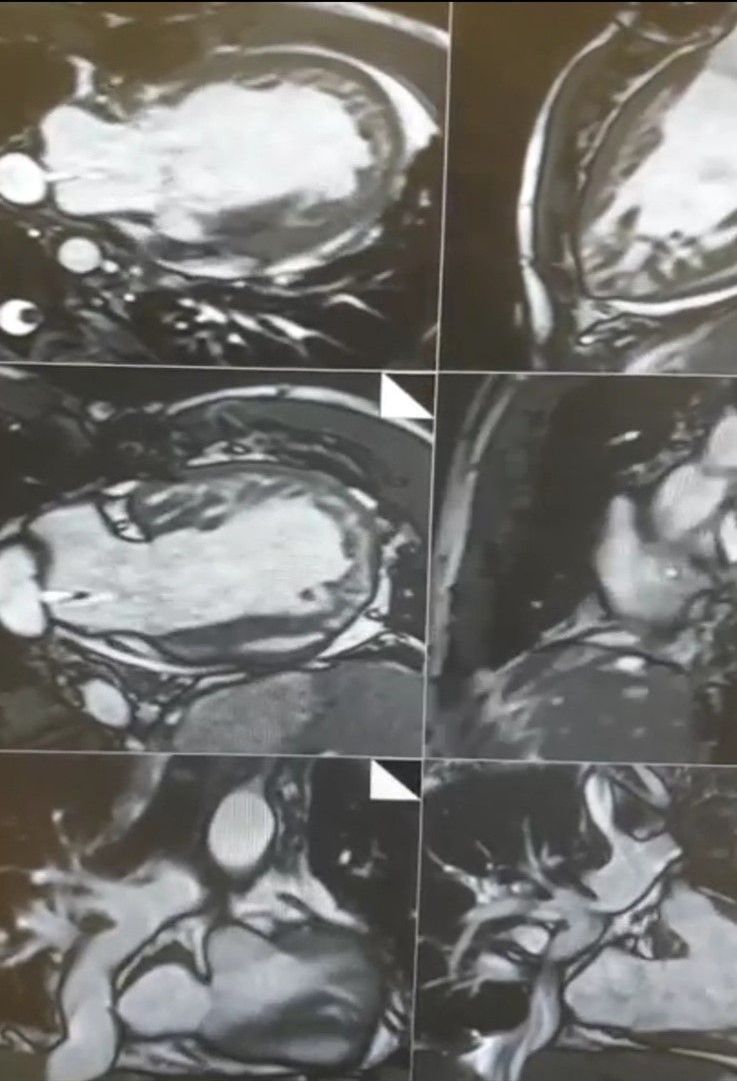
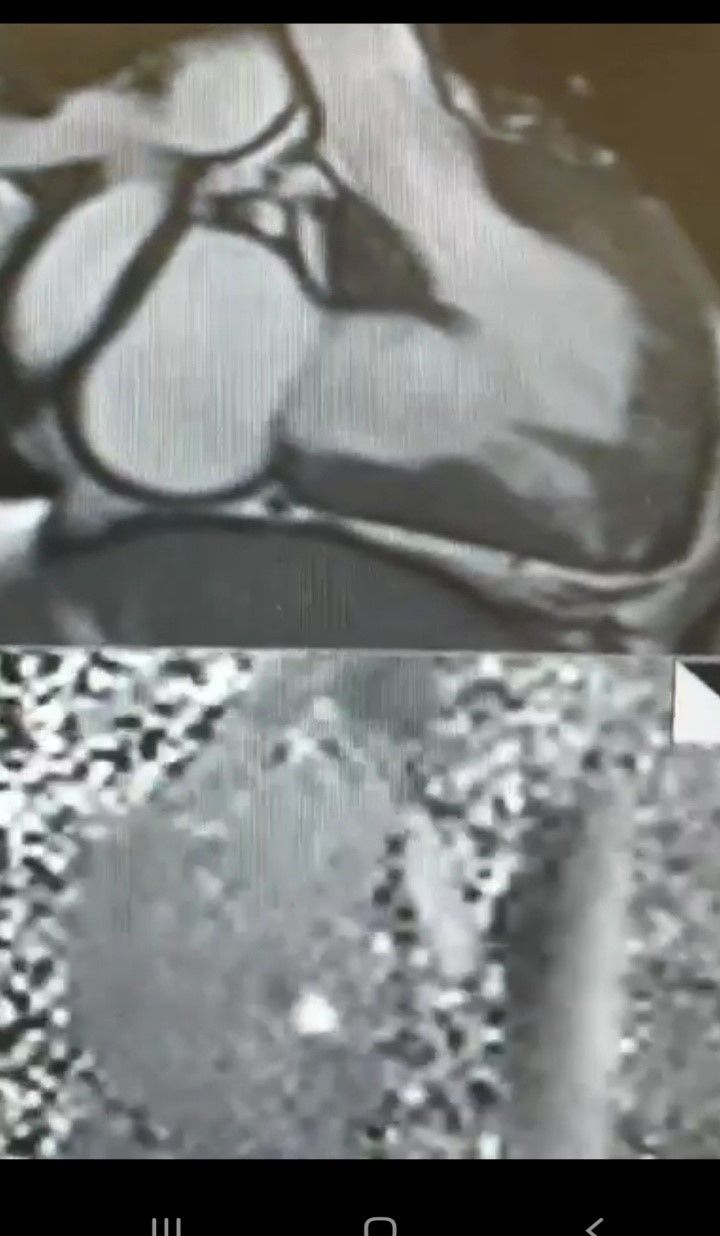
Thrombus, MaR (myocardium at risk) and IV contrast enhanced SSFP cines (CE-SSFP) in cardiac MRI.
It is preferable to do your cines pre-contrast for various reasons,.including, but not limited to, good CNR between myocardium & blood pool. However, doing CE-SSFP does have its advantages. Specifically for thrombus, the thrombus sticks out like a sore thumb and remains jet black on your cine images (as it would on your early gads too), especially if imaged not long after administration of the gadolinium chelate. I also find that CE-SSFP highlights MaR (myocardium at risk) quite well- in that areas at risk become hyperintense (due to the IV contrast) ...correlating to T2 imaging if it has been done well & is free of artefacts. Sometimes CE-SSFP shows up MaR quite well in areas that might not show any late enhancement- which is a good diagnostic indicator (in my view). In this example, I have done my long axis views (2 & 4 chambers) pre-contrast, but my SA post contrast- note the signal of the thrombus and the hyperintense areas of MaR on the CE-SSFP SA- correlating to areas of infarct on the LGE images. Thoughts anyone/everyone?
Amyloid Cardiac MRI
Basic Infiltration Protocol for Amyloid
1. Cine SSFP Long axis & Short axis views
2. Stir/T2 FS Long axis & Short axis views
3. Native MyoMaps (MOLLI) in the Long axis & 3/5 short axis
4. T2 Maps in 3/5 short axis
5. EGE in the Long axis & short axis views
6. PSIR LGE in the long & short axis (you can have the magnitude images included but these will not be of much value as the PSIR)
7. Enhanced MyoMaps in the long axis & short axis views
Look out for the enhancement patterns- depending on the type of amyloid & disease progression. The first clue (for new amyloid diagnosis) should be the lack of 'nulling' on your TI scout/ looklocker- repeat it in a different plane at first, then move straight to PSIR.
Univentricular Fontan MRI with IVC-to-Atria Fenestration
The key to imaging such cardiac anatomy, morphology & function is high-res thin slice SSFP imaging. Key considerations are:
1. Thin slices of about 4 to 6cm
2. Maintaining high SNR through altered voxel size and nex
3. Keeping breath holds short- partial fourier, SFOV, increased segmentation
4. Use of appropriate gating or triggering- if prospective, use view sharing to increase phases & less segments
5. Use of SSh non cine imaging in the 3 orthogonal planes at the start of the scan to identify the anatomy prior to cine imaging- quickens the scan
6. Ensuring that phase flows are positioned appropriately & perpendicular to any jets with the correct venc. May need venc scouts if unsure
7. If needs be, use Hamming filters.